LYMPHANGIOLEIOMYOMATOSIS (LAM)
■Principal investigators
Masaru Suzuki / Department of Respiratory Medicine, Faculty of Medicine and Graduate School of Medicine, Hokkaido University
Toshinori Takada / Uonuma Institute of Community Medicine, Niigata University Medical & Dental Hospital
THERAPEUTIC MECHANISM
Lymphangioleiomyomatosis (LAM) is a rare progressive cystic lung disease, which primarily affects women of childbearing age. When it co-occurs with tuberous sclerosis (TSC), LAM is classified as TSC-LAM and when it occurs in isolation as sporadic LAM; it may also be complicated by angiomyolipoma (AML). In this condition, smooth muscle-like cells (“LAM cells”) multiply in the lungs, producing proteolytic enzymes that destroy lung tissue to form cysts. Since LAM cells also metastasize within the lungs, forming cysts at the resulting metastatic foci, pulmonary function gradually declines, resulting in respiratory failure.
LAM cells exhibit abnormal tuberin and hamartin, two proteins that normally suppress the mammalian target of rapamycin (mTOR) protein. These abnormalities result in constitutive activation of mTOR, causing LAM cells to continue to multiply, triggering the development of LAM.1 Sirolimus exerts its therapeutic effects by inhibiting the activity of mTOR proteins, thereby reducing LAM cell proliferation.
SIROLIMUS’ EFFECTS IN LAM
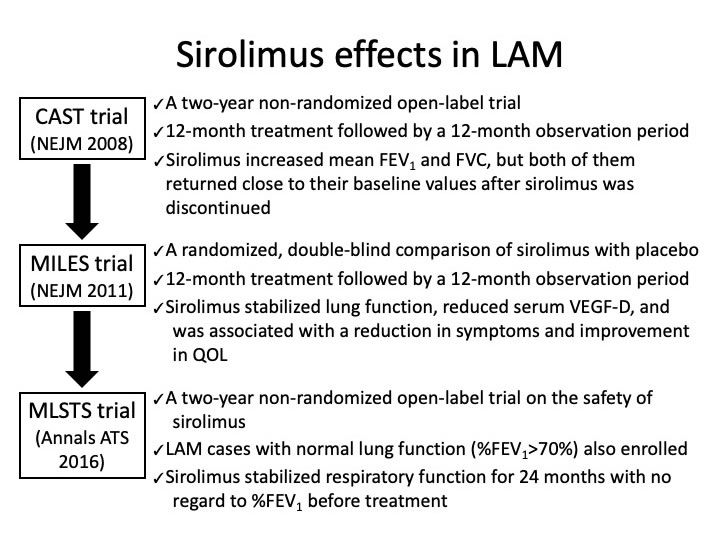
First, a two-year non-randomized open-label trial was conducted in the United States, in which reduction in AML volume was the primary endpoint (CAST trial).2 Sirolimus was taken by 20 patients for one year, who were assessed before and after administration by MRI for imaging features of AML(s) and brain lesions, by CT for lung cysts, and by pulmonary-function testing. Patients’ AMLs shrank by 53.2% on average as a result of one year of sirolimus administration. In addition, in the 11 subjects with comorbid LAM, mean forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) increased respectively by 118 ml and 390 ml, while residual volume decreased by an average of 439 ml. After sirolimus was discontinued, these indicators returned close to their baseline values.
Next, a randomized double-blind trial of LAM patients with moderate or severe pulmonary lesions was conducted, in which the between-group difference in the rate of change of FEV1 was adopted as the primary endpoint (MILES trial).3 Subjects were randomly assigned to one of two groups, taking either sirolimus or placebo for 12 months, and then observed untreated for another 12 months. The monthly FEV1 rate of change was significantly higher in the sirolimus group than in the placebo group (1±2 ml, n=46 v. -12±2 ml, n=43), while FEV1 itself was 153 ml lower in the placebo group than in the sirolimus group. Over the observation period, the sirolimus group’s respiratory function reverted, falling to the same FEV1 rate of change as that of the placebo group.
Later, another study of LAM patients was conducted, this time in Japan: a multicenter trial on the safety of sirolimus administration in LAM patients (MLSTS trial).4 Japanese LAM patients experienced an adverse event profile (i.e., types, frequencies) largely similar to that of the MILES trial, despite taking sirolimus for one year longer; moreover, the study drug’s ability to stabilize respiratory function persisted beyond 12 months in patients with %FEV1 < 70% cases and for the full two years in patients with %FEV1 > 70% cases.
References
1) J Clin Invest 2012;122:3807-3816.
2) N Engl J Med 2008;358:140-151.
3) N Engl J Med 2011;364:1595-1606.
4) Ann Am Thorac Soc 2016;13:1912-1922.
Related Links
LAM is a very rare disease, with an incidence of only 5 per 1 million women of childbearing age. Much remains unclear about the epidemiology of such rare lung diseases in Japan, as little information is available on their diagnosis and treatment. Further, no effective therapies have been established because of the scarcity of information and the lack of clinical opportunities.
For us to gain and apprehend a complete picture of rare lung diseases in Japan, public databases are needed in which confirmed cases can be registered and data accumulated over time. A patient registry for LAM and α1-antitrypsin deficiency has already been started, with the objective of recording data in such a longitudinal fashion, as opposed to cross-sectional ‘snapshots’ in time.
■Rare Lung Disease Registration System | Lymphangioleiomyomatosis and α1-Antitrypsin Deficiency
https://lamaatd.com
On July 4th, 2014, sirolimus became the world’s first drug approved for the treatment of LAM. This prompted the creation of a homepage where visitors can find information related to LAM and sirolimus’ effectiveness in treating it, other sirolimus research, and the journey leading to its regulatory approval, along with relevant research papers and reference materials.
■Clinical Research on Sirolimus for Lymphangioleiomyomatosis (LAM)
http://www.bmrctr.jp/lam/